General Information About Childhood Central Nervous System (CNS) Germ Cell Tumors
Childhood central nervous system (CNS) germ cell tumors form from germ cells.
Germ cells are a type of cell that form as a fetus (unborn baby) develops. These cells later become sperm in the testicles or eggs in the ovaries. Sometimes while the fetus is forming, germ cells travel to other parts of the body and grow into germ cell tumors. Germ cells tumors that form in the brain or spinal cord are called CNS germ cell tumors.
The most common places for one or more central nervous system (CNS) germ cell tumors to form is near the pineal gland and in an area of the brain that includes the pituitary gland and the tissue just above it. Sometimes germ cell tumors may form in other areas of the brain.
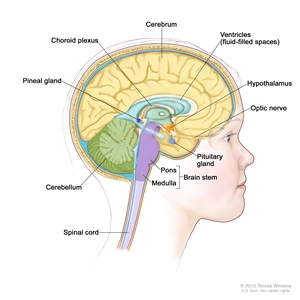
Anatomy of the inside of the brain, showing the pineal and pituitary glands, optic nerve, ventricles (with cerebrospinal fluid shown in blue), and other parts of the brain.
This summary is about germ cell tumors that start in the central nervous system (brain and spinal cord). Germ cell tumors may also form in other parts of the body. See the PDQ summary on Childhood Extracranial Germ Cell Tumors Treatment for information on germ cell tumors that are extracranial (outside the brain).
CNS germ cell tumors usually occur in children, but may occur in adults. Treatment for children may be different than treatment for adults. See the following PDQ summaries for information about treatment for adults:
- Adult Central Nervous System Tumors Treatment
- Extragonadal Germ Cell Tumors Treatment
For information about other types of childhood brain and spinal cord tumors, see the PDQ summary on Childhood Brain and Spinal Cord Tumors Treatment Overview.
There are different types of childhood CNS germ cell tumors.
There are different types of CNS germ cell tumors. The type of CNS germ cell tumor depends on what the cells look like under a microscope. This summary is about the treatment of the following types of CNS germ cell tumors:
Germinomas
Germinomas are the most common type of CNS germ cell tumor and have a good prognosis.
Nongerminomas
Some nongerminomas make hormones. CNS teratomas are a type of nongerminoma that does not make hormones. They may have different kinds of tissue in them, such as hair, muscle, and bone. Teratomas are described as mature or immature, based on how normal the cells look under a microscope. Sometimes teratomas are a mix of mature and immature cells.
Other types of nongerminomas include the following:
- Choriocarcinomas make the hormone beta-human chorionic gonadotropin (β-hCG).
- Embryonal carcinomas do not make hormones.
- Yolk sac tumors make the hormone alpha-fetoprotein (AFP).
- Mixed germ cell tumors are made of more than one kind of germ cell.
The cause of most childhood CNS germ cell tumors is not known.
Signs and symptoms of childhood CNS germ cell tumors include unusual thirst, frequent urination, early puberty, or vision changes.
Signs and symptoms depend on the following:
- Where the tumor has formed.
- The size of the tumor.
- Whether the tumor makes hormones.
Signs and symptoms may be caused by childhood CNS germ cell tumors or by other conditions. Check with your child's doctor if your child has any of the following:
- Being very thirsty.
- Making large amounts of urine that is clear or almost clear.
- Frequent urination.
- Bed wetting or getting up at night to urinate.
- Trouble moving the eyes or trouble seeing clearly.
- Loss of appetite.
- Weight loss for no known reason.
- Early or late puberty.
- Short stature (being shorter than normal).
- Headaches.
- Nausea and vomiting.
- Feeling very tired.
- Having problems with school work.
Imaging studies and tests are used to detect (find) and diagnose childhood CNS germ cell tumors.
The following tests and procedures may be used:
- Physical exam and history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient's health habits and past illnesses and treatments will also be taken.
- Neurological exam: A series of questions and tests to check the brain, spinal cord, and nerve function. The exam checks a person's mental status, coordination, and ability to walk normally, and how well the muscles, senses, and reflexes work. This may also be called a neuro exam or a neurologic exam.
- Visual field exam: An exam to check a person's field of vision (the total area in which objects can be seen). This test measures both central vision (how much a person can see when looking straight ahead) and peripheral vision (how much a person can see in all other directions while staring straight ahead). The eyes are tested one at a time. The eye not being tested is covered.
- MRI (magnetic resonance imaging) with gadolinium: A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the brain and spinal cord. A substance called gadolinium is injected into a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- Lumbar puncture: A procedure used to collect cerebrospinal fluid (CSF) from the spinal column. This is done by placing a needle between two bones in the spine and into the CSF around the spinal cord and removing a sample of the fluid. The sample of CSF is checked under a microscope for signs of tumor cells. The sample may also be checked for the amounts of protein and glucose. A higher than normal amount of protein or lower than normal amount of glucose may be a sign of a tumor. This procedure is also called an LP or spinal tap.
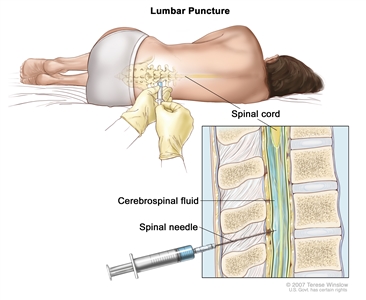
Lumbar puncture. A patient lies in a curled position on a table. After a small area on the lower back is numbed, a spinal needle (a long, thin needle) is inserted into the lower part of the spinal column to remove cerebrospinal fluid (CSF, shown in blue). The fluid may be sent to a laboratory for testing. - Tumor marker tests: A procedure in which a sample of blood or cerebrospinal fluid (CSF) is checked to measure the amounts of certain substances released into the blood and CSF by organs, tissues, or tumor cells in the body. Certain substances are linked to specific types of cancer when found in increased levels in the blood. These are called tumor markers. The following tumor markers are used to diagnose some CNS germ cell tumors:
- Alpha-fetoprotein (AFP).
- Beta-human chorionic gonadotropin (β-hCG).
- Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. An unusual (higher- or lower-than-normal) amount of a substance can be a sign of disease.
- Blood hormone studies: A procedure in which a blood sample is checked to measure the amounts of certain hormones released into the blood by organs and tissues in the body. An unusual (higher- or lower-than-normal) amount of a substance can be a sign of disease in the organ or tissue that makes it. The blood will be checked for the levels of hormones made by the pituitary gland and other glands.
A biopsy may be done to be sure of the diagnosis of CNS germ cell tumor.
If doctors think your child may have a CNS germ cell tumor, a biopsy may be done. For brain tumors, the biopsy is done by removing part of the skull and using a needle to remove a sample of tissue. Sometimes, a needle guided by a computer is used to remove the tissue sample. A pathologist views the tissue under a microscope to look for cancer cells. If cancer cells are found, the doctor may remove as much tumor as safely possible during the same surgery. The piece of skull is usually put back in place after the procedure.
Sometimes the diagnosis can be made based on the results of imaging and tumor marker tests and a biopsy is not needed.
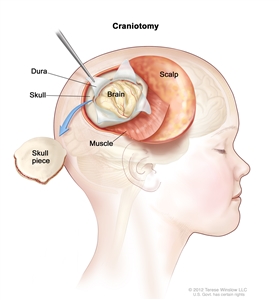
Craniotomy: An opening is made in the skull and a piece of the skull is removed to show part of the brain.
The following test may be done on the sample of tissue that is removed:
- Immunohistochemistry: A test that uses antibodies to check for certain antigens in a sample of tissue. The antibody is usually linked to a radioactive substance or a dye that causes the tissue to light up under a microscope. This type of test may be used to tell the difference between different types of brain tumors.
Certain factors affect prognosis (chance of recovery).
The prognosis (chance of recovery) depends on the following:
- The type of germ cell tumor.
- The type and level of any tumor markers.
- Where the tumor is in the brain or in the spinal cord.
- Whether the cancer has spread within the brain and spinal cord or to other parts of the body.
- Whether the tumor is newly diagnosed or has recurred (come back) after treatment.
Stages of Childhood CNS Germ Cell Tumors
Childhood central nervous system (CNS) germ cell tumors rarely spread outside of the brain and spinal cord.
Staging is the process used to find out how much cancer there is and if cancer has spread. There is no standard staging system for childhood central nervous system (CNS) germ cell tumors. The treatment plan depends on the following:
- The type of germ cell tumor.
- Whether the tumor has spread within the CNS or to other parts of the body.
- The results of tests and procedures done to diagnose childhood CNS germ cell tumors.
- Whether the tumor is newly diagnosed or has recurred (come back) after treatment.
Recurrent Childhood CNS Germ Cell Tumors
Childhood central nervous system germ cell tumors may recur (come back) after they have been treated. The tumors usually come back in the same place as the first tumor. The tumor also may come back in other places and/or in the meninges (thin layers of tissue that cover and protect the brain and spinal cord).
Treatment Option Overview
There are different types of treatment for patients with childhood central nervous system (CNS) germ cell tumors.
Different types of treatment are available for children with childhood central nervous system (CNS) germ cell tumors. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment.
Because cancer in children is rare, taking part in a clinical trial should be considered. Some clinical trials are open only to patients who have not started treatment.
Children with childhood CNS germ cell tumors should have their treatment planned by a team of health care providers who are experts in treating cancer in children.
Treatment will be overseen by a pediatric oncologist and/or a radiation oncologist,. A pediatric oncologist is a doctor who specializes in treating children with cancer. A radiation oncologist specializes in treating cancer with radiation therapy. These doctors work with other pediatric health care providers who are experts in treating children with childhood CNS germ cell tumors and who specialize in certain areas of medicine. These may include the following specialists:
- Pediatrician.
- Pediatric neurosurgeon.
- Neurologist.
- Endocrinologist.
- Ophthalmologist.
- Pediatric nurse specialist.
- Rehabilitation specialist.
- Psychologist.
- Social worker.
Childhood CNS germ cell tumors may cause signs or symptoms that begin before the cancer is diagnosed and continue for months or years.
Childhood CNS germ cell tumors may cause signs or symptoms that continue for months or years. Signs or symptoms caused by the tumor may begin before the cancer is diagnosed. Signs or symptoms caused by treatment may begin during or right after treatment.
Some cancer treatments cause side effects months or years after treatment has ended.
Some cancer treatments cause side effects that continue or appear months or years after cancer treatment has ended. These are called late effects. Late effects of cancer treatment may include:
- Physical problems.
- Changes in mood, feelings, thinking, learning, or memory.
- Second cancers (new types of cancer).
Some late effects may be treated or controlled. It is important to talk with your child's doctors about the possible late effects caused by some treatments. (See the PDQ summary on Late Effects of Treatment for Childhood Cancer for more information).
Four types of treatment are used:
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy:
- External radiation therapy uses a machine outside the body to send radiation toward the cancer. Certain ways of giving radiation therapy can help keep radiation from damaging nearby healthy tissue. This type of radiation therapy may include the following:
- Stereotactic radiosurgery: Stereotactic radiosurgery is a type of external radiation therapy. A rigid head frame is attached to the skull to keep the head still during the radiation treatment. A machine aims a single large dose of radiation directly at the tumor. This procedure does not involve surgery. It is also called stereotaxic radiosurgery, radiosurgery, and radiation surgery.
- Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer.
The way the radiation therapy is given depends on the type of cancer being treated.
External radiation therapy is used to treat childhood CNS germ cell tumors. Radiation therapy to the brain can affect growth and development in young children. Certain ways of giving radiation therapy can lessen the damage to healthy brain tissue. For children younger than 3 years, chemotherapy may be given instead. This can delay or reduce the need for radiation therapy.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). The way the chemotherapy is given depends on the type of cancer being treated.
Surgery
Whether surgery to remove the tumor can be done depends on where the tumor is in the brain. Surgery to remove the tumor may cause severe, long-term side effects.
Surgery may be done to remove teratomas and may be used for germ cell tumors that come back. Even if the doctor removes all the cancer that can be seen at the time of the surgery, some patients may be given chemotherapy or radiation therapy after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
High-dose chemotherapy with stem cell rescue
High-dose chemotherapy with stem cell rescue is a way of giving high doses of chemotherapy and replacing blood -forming cells destroyed by the cancer treatment. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient or a donor and are frozen and stored. After the chemotherapy is completed, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body's blood cells.
New types of treatment are being tested in clinical trials.
Information about clinical trials is available from the NCI website.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. See the Current Clinical Trials section that follows for links to current treatment clinical trials. These have been retrieved from the NCI's listing of clinical trials.
Follow-up tests may be needed.
Some of the tests that were done to diagnose the cancer or to find out the stage of the cancer may be repeated. Some tests will be repeated in order to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your child's condition has changed or if the cancer has recurred (come back). These tests are sometimes called follow-up tests or check-ups.
Children whose cancer affected their pituitary gland when the cancer was diagnosed will usually need to have their blood hormone levels checked. If the blood hormone level is low, replacement hormone medicine is given.
Children who had a high tumor marker level (alpha-fetoprotein or beta-human chorionic gonadotropin) when the cancer was diagnosed usually need to have their blood tumor marker level checked. If the tumor marker level increases after initial treatment, the tumor may have recurred.
Treatment Options for Childhood CNS Germ Cell Tumors
Newly Diagnosed CNS Germinomas
Treatment of newly diagnosed central nervous system (CNS) germinomas may include the following:
- Radiation therapy to the tumor and ventricles (fluid -filled spaces) of the brain. A higher dose of radiation is given to the tumor than the area around the tumor.
- Chemotherapy followed by radiation therapy, for younger children.
- A clinical trial of chemotherapy followed by radiation therapy given in lower doses depending on how the tumor responds to treatment.
Newly Diagnosed CNS Teratomas
Treatment of newly diagnosed mature and immature central nervous system (CNS) teratomas may include the following:
- Surgery to remove as much of the tumor as possible. Radiation therapy and/or chemotherapy may be given if any tumor remains after surgery.
Newly Diagnosed CNS Nongerminomas
It is not clear what treatment is best for newly diagnosed central nervous system (CNS) nongerminomas is. Treatment of choriocarcinoma, embryonal carcinoma, yolk sac tumor, or mixed germ cell tumor may include the following:
- Chemotherapy followed by radiation therapy. If a mass remains after chemotherapy, surgery may be needed to check if the mass is a mature teratoma, fibrosis, or a growing tumor.
- If the mass is a mature teratoma or fibrosis, radiation therapy is given.
- If the mass is a growing tumor, other treatments may be given.
- Surgery to remove as much of the mass as possible and check for tumor cells, if tumor marker levels are normal and the mass continues to grow (called growing teratoma syndrome).
- A clinical trial of chemotherapy followed by radiation therapy given in lower doses depending on how the tumor responds to treatment.
Recurrent Childhood CNS Germ Cell Tumors
Treatment of recurrent childhood central nervous system (CNS) germ cell tumors may include the following:
- Chemotherapy followed by radiation therapy.
- High-dose chemotherapy with stem cell rescue using the patient's stem cells.
- A clinical trial of a new treatment.
Current Clinical Trials
Check the list of NCI-supported cancer clinical trials that are now accepting patients with childhood central nervous system germ cell tumor. For more specific results, refine the search by using other search features, such as the location of the trial, the type of treatment, or the name of the drug. Talk with your child's doctor about clinical trials that may be right for your child. General information about clinical trials is available from the NCI website.
To Learn More About Childhood CNS Germ Cell Tumors
For more information about childhood central nervous system germ cell tumors, see the following:
- What You Need to Know About™ Brain Tumors
- Pediatric Brain Tumor Consortium (PBTC)
For more childhood cancer information and other general cancer resources, see the following:
- About Cancer
- Childhood Cancers
- CureSearch for Children's Cancer
- Late Effects of Treatment for Childhood Cancer
- Adolescents and Young Adults with Cancer
- Children with Cancer: A Guide for Parents
- Cancer in Children and Adolescents
- Staging
- Coping with Cancer
- Questions to Ask Your Doctor about Cancer
- For Survivors and Caregivers
About This PDQ Summary
About PDQ
Physician Data Query (PDQ) is the National Cancer Institute's (NCI's) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government's center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the treatment of childhood central nervous system germ cell tumors. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary ("Date Last Modified") is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Pediatric Treatment Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become "standard." Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials are listed in PDQ and can be found online at NCI's website. Many cancer doctors who take part in clinical trials are also listed in PDQ. For more information, call the Cancer Information Service 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as "NCI's PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary]."
The best way to cite this PDQ summary is:
PDQ® Pediatric Treatment Editorial Board. PDQ Childhood Central Nervous System Germ Cell Tumors Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: https://www.cancer.gov/types/brain/patient/child-cns-germ-cell-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389502]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 2,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website's E-mail Us.
Last Revised: 2016-08-29
If you want to know more about cancer and how it is treated, or if you wish to know about clinical trials for your type of cancer, you can call the NCI's Cancer Information Service at 1-800-422-6237, toll free. A trained information specialist can talk with you and answer your questions.